

X

API Suppliers

US DMFs Filed

CEP/COS Certifications

JDMFs Filed
Other Certificates
Other Suppliers
USA (Orange Book)
Europe

Canada

Australia

South Africa
Uploaded Dossiers
U.S. Medicaid
Annual Reports
Impressions: 2622
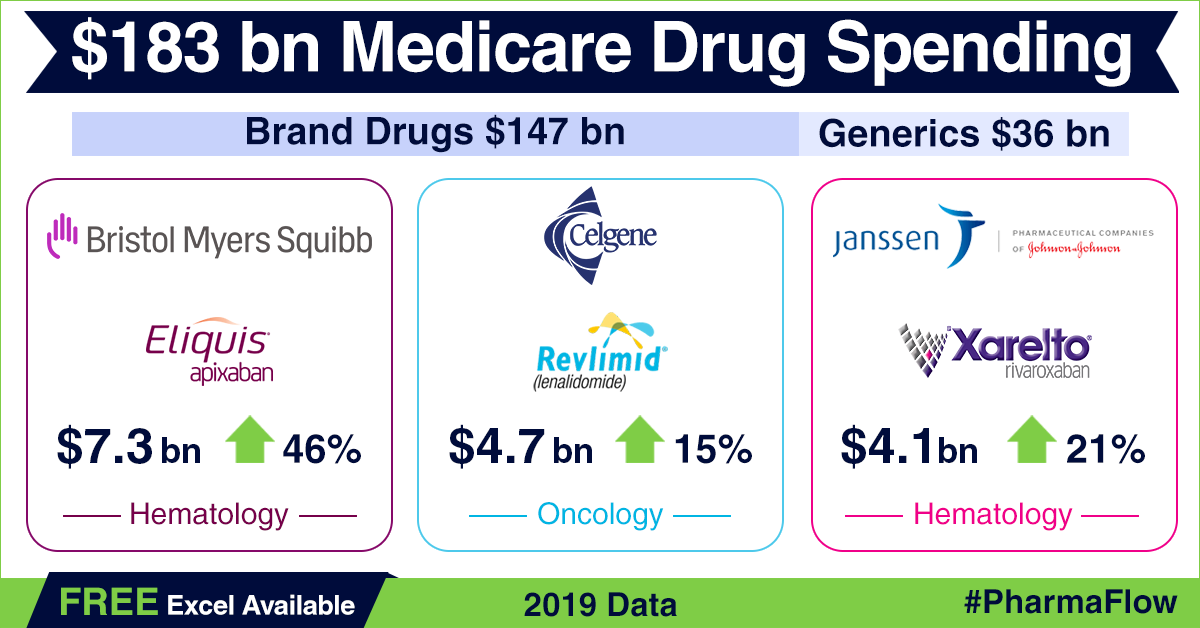
https://www.pharmacompass.com/radio-compass-blog/america-s-drug-price-hike-conundrum-in-backdrop-of-2019-medicare-part-d-data
Impressions: 2500
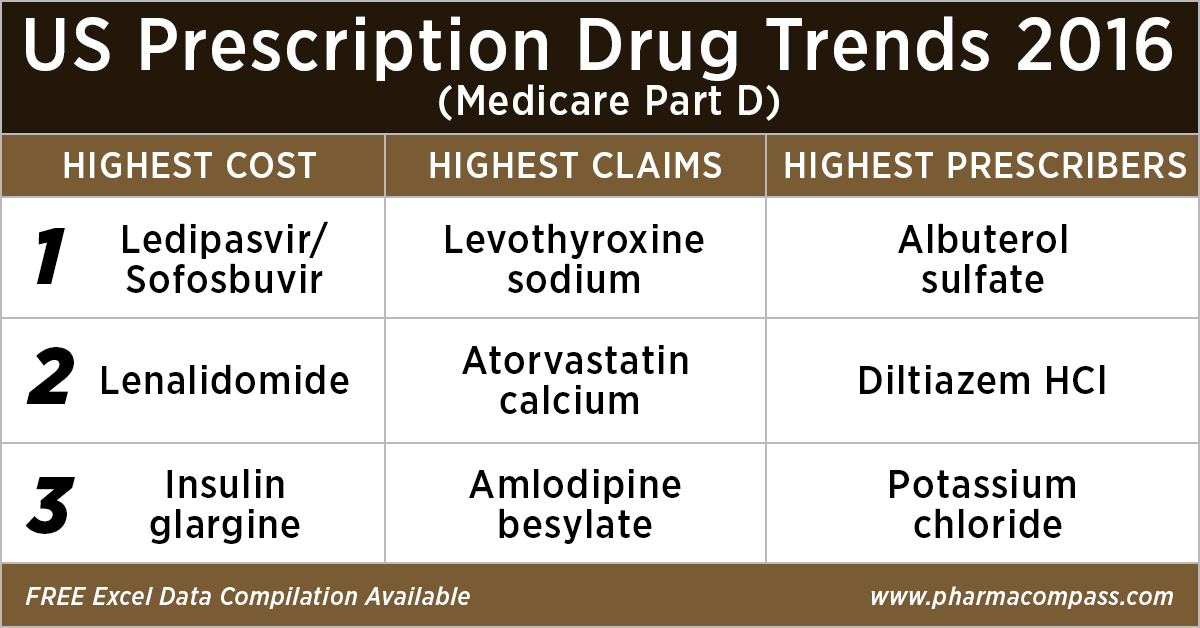
https://www.pharmacompass.com/radio-compass-blog/analyzing-over-us-90-billion-of-medicare-prescription-drug-part-d-spending-in-2016

Impressions: 3525
https://www.pharmacompass.com/radio-compass-blog/divi-s-labs-on-fda-s-import-alert-list-but-did-it-refuse-an-inspection

Impressions: 5513
https://www.pharmacompass.com/radio-compass-blog/teva-ceo-steps-down-fda-warning-letters-to-firms-in-japan-india-china

Impressions: 7923
https://www.pharmacompass.com/radio-compass-blog/drug-costs-and-prescription-trends-in-the-united-states-analyzing-medicare-s-121-billion-spend

Impressions: 4476
https://www.pharmacompass.com/radio-compass-blog/china-shuts-plants-of-major-antibiotic-producers-to-fight-pollution-more-troubles-for-teva







