

X

API Suppliers

US DMFs Filed

CEP/COS Certifications
0

JDMFs Filed
Other Certificates
Other Suppliers
USA (Orange Book)
Europe

Canada

Australia
0

South Africa
Uploaded Dossiers
U.S. Medicaid
Annual Reports
0
Impressions: 2500
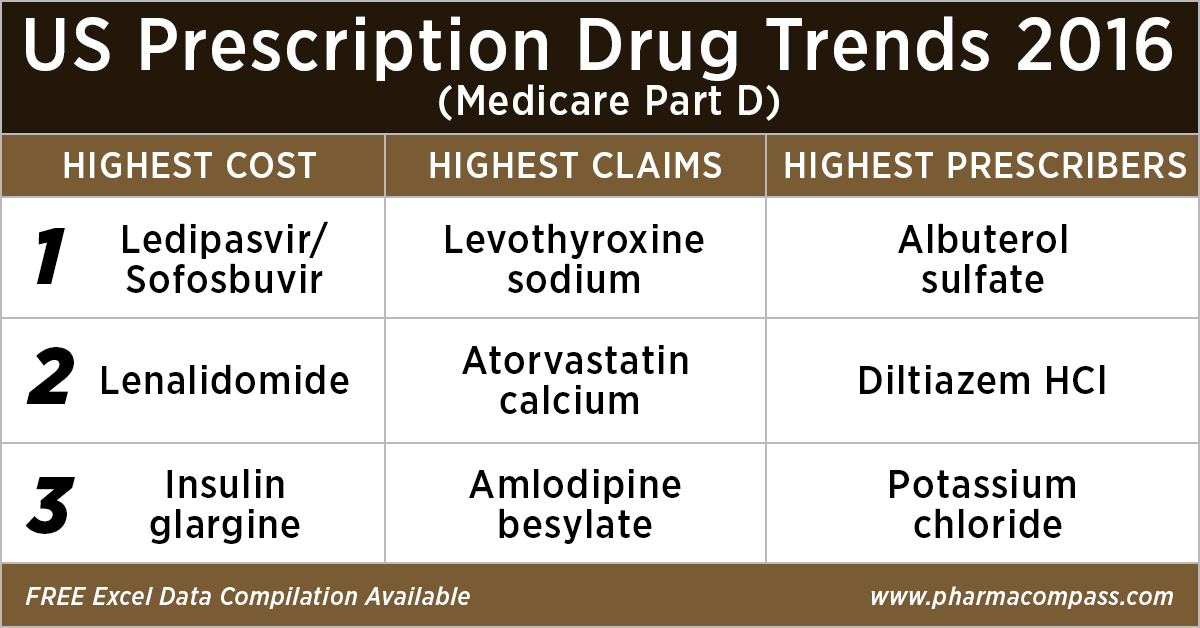
https://www.pharmacompass.com/radio-compass-blog/analyzing-over-us-90-billion-of-medicare-prescription-drug-part-d-spending-in-2016

Impressions: 9420
https://www.pharmacompass.com/radio-compass-blog/eu-suspends-drugs-from-granules-indian-facility-where-fda-had-no-concerns

Impressions: 7923
https://www.pharmacompass.com/radio-compass-blog/drug-costs-and-prescription-trends-in-the-united-states-analyzing-medicare-s-121-billion-spend

Impressions: 7491
https://www.pharmacompass.com/radio-compass-blog/novartis-plant-shut-down-creates-urgency-to-find-alternatives-to-chinese-apis







