






This week, PharmaCompass
reviews the recently released data on prescription drugs paid for under the
Medicare Part D Prescription Drug Program in the United States in calendar year
2016.
But first, let’s understand what is Medicare.
Medicare is the federal health insurance program in the US. In 2017, it covered 58.4 million people — 49.5 million aged 65 and older, and 8.9 million disabled.
Prescription drug coverage under this
program was started in 2006, and is known as Medicare Part D.
As part of this
coverage, the Centers for Medicare & Medicaid Services (CMS) contracts insurance
companies and other private companies, known as plan sponsors, that offer
prescription drug plans to their beneficiaries with varying drug coverage and
cost-sharing requirements.
In
2017, the Congressional Budget Office (CBO) had estimated that spending on
Medicare Part D would reach US$ 94 billion, or about 16 percent of all Medicare
expenditures for the year.
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
According
to the CBO, Medicare Part D is the most significant expansion of the Medicare
program since it was created by Congress in 1965.
With
more than 1.48 billion claims from beneficiaries enrolled under the Part D
prescription drug benefit program under its umbrella, our analysis of Medicare
Part D provides valuable insights into how elderly Americans use prescription
drugs.
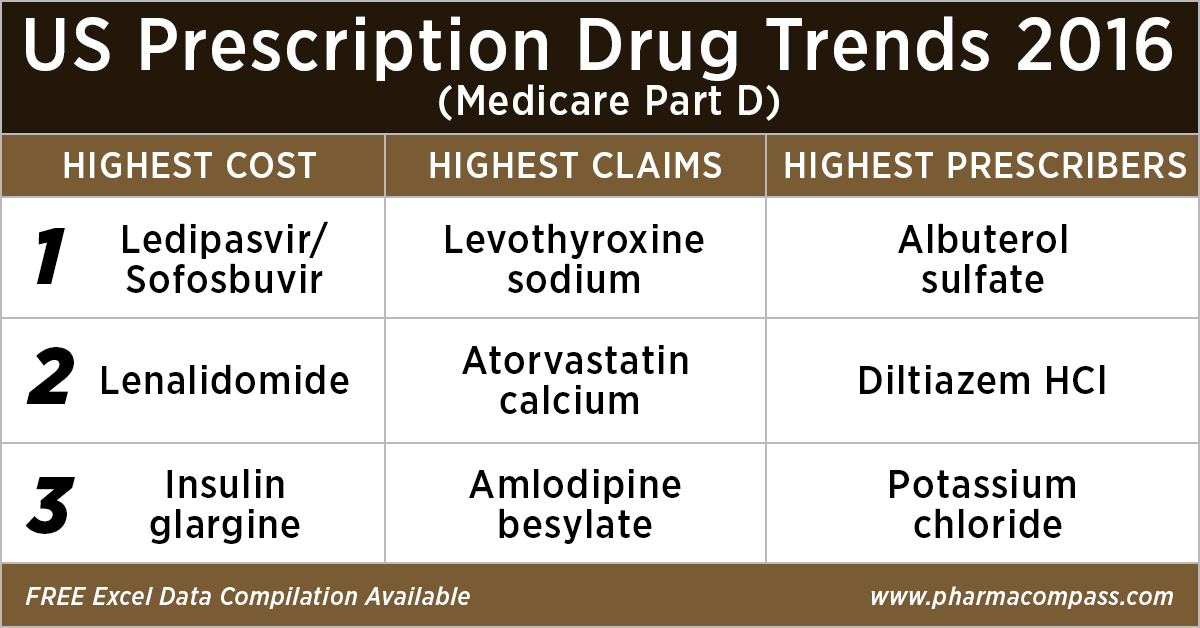
Top 10 drugs by
cost: The ones that bore the highest cost burden for Medicare
As in 2015, in 2016
too Gilead’s Hepatitis C treatment — Ledipasvir/Sofosbuvir (Harvoni) — remained the single drug highest payout under the Medicare Part D Prescription Drug Program with a total cost of US$ 4.4 billion.
As Gilead continued
to face competition from AbbVie and Merck in the Hepatitis C space, the spending on Harvoni was down
37 percent from US$ 7.03 billion in 2015.
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
Celgene’s cancer treatment, Lenalidomide (Revlimid), Sanofi and Merck’s diabetes treatments and AstraZeneca’s Crestor (Rosuvastatin Calcium) for
cholesterol followed Harvoni. All together, they cost the Medicare program over US$ 10 billion.
Generic Name
Number of Medicare Part D Claims
Number of Medicare Beneficiaries
Number of Prescribers
Aggregate Cost Paid for Part D
Claims (In USD)
LEDIPASVIR/ SOFOSBUVIR (HARVONI)
141,665
52,782
12,097
4,398,534,465
LENALIDOMIDE
239,049
35,368
10,382
2,661,106,127
LANTUS SOLOSTAR (INSULIN
GLARGINE, HUM.REC.ANLOG )
5,028,485
1,075,248
245,447
2,526,048,766
SITAGLIPTIN PHOSPHATE
4,742,505
864,442
206,223
2,440,013,513
ROSUVASTATIN CALCIUM
6,012,444
1,560,050
249,981
2,322,724,007
FLUTICASONE/SALMETEROL
5,194,391
1,196,007
275,442
2,319,808,482
PREGABALIN
4,940,115
852,497
267,532
2,098,953,250
RIVAROXABAN
4,403,332
807,820
252,141
1,954,748,890
APIXABAN
4,455,782
826,969
231,631
1,926,107,484
TIOTROPIUM BROMIDE
4,153,162
903,494
235,564
1,818,857,361
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
Top 10 drugs by claims: The most commonly
used drugs of 2016
With 46.6 million claims, the thyroid hormone deficiency treatment — Levothyroxine Sodium — retained its position of being the most claimed product under Medicare’s Part D Prescription Drug Program in 2016.
The number of
Medicare Part D claims includes original prescriptions and refills.
Following Levothyroxine Sodium was the lipid-lowering agent — Atorvastatin Calcium — which had 44.5 million Medicare Part D claims that
were filed by almost 9.4 million beneficiaries.
Generic
Name
Number
of Prescribers
Number
of Medicare Part D Claims
Number
of Medicare Beneficiaries
LEVOTHYROXINE SODIUM
669,999
46,617,109
8,091,785
ATORVASTATIN CALCIUM
494,973
44,595,686
9,435,633
AMLODIPINE BESYLATE
497,017
39,913,468
7,802,905
LISINOPRIL
490,452
39,469,840
8,009,954
OMEPRAZOLE
492,951
32,909,236
7,001,160
METFORMIN HCL
611,700
31,007,932
6,394,014
SIMVASTATIN
380,560
29,687,947
6,201,911
HYDROCODONE/ACETAMINOPHEN
660,617
28,595,150
7,265,882
FUROSEMIDE
488,352
27,878,243
5,421,598
GABAPENTIN
555,997
27,627,466
5,363,382
Click here
to access the compilation of Medicare Part D Prescriber Summary Report
Top 10 drugs by prescribers: Medicines that were most popular with
doctors
Among the prescribers, albuterol sulfate (salbutamol) and Diltiazem had
over 900,000 unique providers (or
doctors) prescribing the drug.
Albuterol (salbutamol) is
used to provide quick relief from wheezing and shortness
of breath while Diltiazem is used to prevent chest
pain (angina).
Also
on the list of popular drugs with prescribers is Hydrocodone-Acetaminophen.
With more doctors prescribing Hydrocodone-Acetaminophen (an
opioid) than commonly used antibiotics, such as Cephalexin, Ciprofloxacin and Amoxicillin, the
series of new FDA initiatives to combat the epidemic of opioid misuse and abuse
should change the position of opioids in the top 10 drugs by prescribers in the
coming years.
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
Generic
Name
Number of
Prescribers
Number of
Medicare Part D Claims
Number of
Medicare Beneficiaries
ALBUTEROL SULFATE
985,427
13,100,354
5,417,718
DILTIAZEM HCL
931,159
8,142,004
1,982,550
POTASSIUM CHLORIDE
879,491
18,945,969
4,278,000
PEN NEEDLE, DIABETIC
677,210
5,281,778
1,795,046
LEVOTHYROXINE SODIUM
669,999
46,617,109
8,091,785
HYDROCODONE/ACETAMINOPHEN
660,617
28,595,150
7,265,882
METFORMIN HCL
611,700
31,007,932
6,394,014
CEPHALEXIN
597,647
5,603,879
3,933,373
CIPROFLOXACIN HCL
594,129
7,000,081
4,851,657
AZITHROMYCIN
591,028
7,958,625
5,734,122
What does the
future hold?
Although the Part D Prescriber PUF (public use file) has a wealth of information on payment and utilization for Medicare Part D prescriptions, the dataset has a number of limitations. Of particular importance is the fact that the data may not be representative of a physician’s entire practice or all of Medicare as it only includes information on beneficiaries enrolled in the Medicare Part D prescription drug program (i.e., approximately two-thirds of all Medicare beneficiaries).
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
Last
month, the Office of the Inspector General (OIG)
reviewed
the Part D claims data for the years 2011 to 2015 for brand-name drugs.
The OIG’s report found that the total reimbursement for all brand-name drugs in Part D increased 77 percent from 2011 to 2015, despite a 17-percent decrease in the number of prescriptions for these drugs.
With soaring drug prices being an issue for
regular debate in the Unites States and President Trump announcing that his
team will use strategies to strengthen the negotiating powers under
Medicare Part D and Part B, it remains to be seen how the data on prescription drugs paid for under
the Medicare Part D Prescription Drug Program will change in the coming years.
Click here to access the compilation of Medicare Part D
Prescriber Summary Report
Impressions: 2500
https://www.pharmacompass.com/radio-compass-blog/analyzing-over-us-90-billion-of-medicare-prescription-drug-part-d-spending-in-2016
#PharmaFlow by PHARMACOMPASS
05 Jul 2018

In October
2016, the US Food and Drug Administration (FDA) inspected a facility in India
belonging to Granules India that manufactures pharmaceutical
formulation intermediates (PFIs) and finished dosage forms (FDFs). The FDA had
no observations.
Three months later, Portugal’s health authority — INFARMED — inspected the same site and detected non-conformities in good manufacturing practices (GMPs).
According to an alert published
on the INFARMED website, the observations were related to granulation and
primary packaging of tablets in batches of drugs related to paracetamol and metformin supplied by Granules to Mylan, Bluepharma and Sandoz. The agency recommended the
suspension and recall of certain batches from the market in Portugal.
Last week, based on “General GMP Observations” of “regulatory partner(s)”, Health Canada placed Granules India’s facility located in Gagillapur (near Hyderabad) on its inspection tracker. Health Canada’s inspection tracker provides updates on the actions the regulator is undertaking to assess and manage potential risks arising from inspections of drug manufacturing facilities.
According to
Granules, their facility in Gagillapur contributes over 50 percent to their revenues and “has the world’s largest PFI capacity along with an industry-leading batch size of six tons. In addition, the Gagillapur facility has one of the largest single-site finished dosage capacities in the world for their respective products.”
In a recent
interview, C. Krishna Prasad, managing director of Granules India, said there
were no issues related to data integrity and INFARMED is scheduled to re-inspect
the Gagillapur facility this week.
Data
integrity concerns at ACS Dobfar’s
Italian facility
The FDA’s April 2016 inspection of ACS Dobfar’s
operations in Brazil — Antibioticos do Brasil (ABL) — led to the issuance of a warning letter in December. Among other observations, the FDA investigators found that the filling zone for sterile injectable product was not sufficiently robust. Therefore, it didn’t protect the drugs being manufactured there (such as during the times when operators entered the final filling area).
Almost immediately after the warning letter was issued, an inspection of the same facility by the Italian Regulatory Agency (AIFA) found it not-compliant for the manufacture of the active ingredient — Cephalexin Sodium Sterile. AIFA also recommended the
suspension of the Certificate of Suitability issued for ceftazidime pentahydrate with sodium carbonate for injection.
The inspectors
found ABL failed to ensure a good level of maintenance and cleaning of the
final crystallization area and there was a poor level of training, low
knowledge and awareness of good manufacturing practices (GMP) along with lack of supervisory
control.
The
non-compliance report also mentions that some non-authorized and fraudulent
activities were stopped before inspectors entered certain manufacturing areas.
Fraudulent activities were not limited to Brazil, as ACS Dobfar’s Italian drug manufacturing facility — FACTA Farmaceutici SpA — had FDA investigators uncover data-integrity violations during a January 2016 inspection.
The warning
letter issued to FACTA mentions that for multiple lots of sterile drug product,
where the original data showed failing results, the data reportedly showed
passing results.
The company was found storing original data in an “unofficial” and uncontrolled electronic spreadsheet on a shared computer network drive. The analyst told investigators that original data was first recorded in the “unofficial” spreadsheet and later transcribed to an “official” form.
Investigators also observed many
copies of uncontrolled blank and partially-completed cGMP forms and also
documented that employees at FACTA used paper shredders to destroy critical
laboratory and production records.
It is worth mentioning that FACTA’s EU GMP certification was renewed by the Italian regulators after an inspection that was conducted at the same time as the FDA inspection.
Data integrity concerns confirmed at Divi’s Laboratories in India
Divi’s Laboratories’ Unit-II situated in Visakhapatnam, Andhra Pradesh — one of the biggest manufacturing facilities for the major producer of active pharmaceutical ingredients (APIs) — was inspected by the US FDA from November 29 to December 6, 2016.
The regulators
issued a Form 483 with five observations.
While data integrity concerns had been widely reported in news media,
Health Canada confirmed the violations by placing the company on its inspection
tracker last week.
FDA’s warning letter comes to haunt Dr. Reddy’s
South Korean biotech firm — Mezzion Inc — filed a suit for damages
against Dr. Reddy’s in New Jersey state court alleging that it hid “significant deficiencies in its FDA cGMP practices” and misrepresented its compliance.
Mezzion has stated in its suit that “Dr. Reddy's repeatedly represented to Mezzion that it was compliant with FDA regulations” whereas the FDA issued a warning letter to Dr. Reddy's.
During an FDA inspection at Dr. Reddy's facilities in India, the FDA identified numerous data integrity violations and also uncovered a previously unknown and uncontrolled “Custom QC laboratory” (CQC), which engaged in a “practice of substituting repeat tests after failing results.”
Mezzion further states: “Dr. Reddy’s misconduct was the sole reason given by the FDA to deny approval of Mezzion’s new drug application (NDA) for udenafil for the treatment of erectile dysfunction (ED)”. As a result, Mezzion has incurred delays and was forced to seek new manufacturers and suppliers for udenafil and the udenafil finished product, in order to resubmit its udenafil New Drug Application (NDA) to the FDA for approval.
FDA’s warning letters to
manufacturers in UK and India
Porton Biopharma, UK: A
warning letter was
issued to the UK-based Porton Biopharma by the US FDA for manufacturing violations related to Erwinaze (asparaginase Erwinia chrysanthemi) — an orphan biologic which was developed by Porton and licensed to Jazz Pharmaceuticals.
According to the warning letter, the FDA had previously performed an inspection of Porton’s facility in January 2015 and found similar concerns. The inspection between March 7 and 18, 2016,
which triggered the warning letter,
had FDA investigators observe continued deficiencies, including metal particles
which penetrated a few batches of Erwinaze, another batch containing paper or
cardboard fibers and a possible microbial contamination.
While Porton
believed that vial stoppers were the source of the metal scraps, the FDA
investigators were not convinced.
Erwinaze
generated around US $ 43 million in the third quarter for Jazz Pharmaceuticals, accounting for more than 10 percent of the company’s revenues.
CTX Life Sciences, India: The FDA issued a warning letter to CTX Life Sciences in India after making observations of rust, insects, damaged interiors, and/or drug residues in pieces of manufacturing equipment identified as “clean”.
Investigators also found that the API were released without testing because the necessary laboratory equipment was out of order. While the company had decided to release batches “on conditional basis and as soon as UV maintenance issue rectified analysis shall be performed” the investigators could find no trace of the testing.
Our view
Last week, in
our compliance round up, we had reported the shredding of documents at Hetero Labs in India. And this week, similar issues have surfaced in
Italy.
It’s clear that corrupt practices of data integrity are spreading across the industry and are no longer confined to a region.
At the same time, while both European and US regulators reached a similar outcome on the compliance status of Antibioticos do Brasil, the divergent views at Granules India and FACTA Farmaceutici indicate the urgency for regulators to establish a consistent global evaluation standard for pharmaceutical manufacturing.
Impressions: 9420
https://www.pharmacompass.com/radio-compass-blog/eu-suspends-drugs-from-granules-indian-facility-where-fda-had-no-concerns
#PharmaFlow by PHARMACOMPASS
02 Feb 2017

In less than three weeks, Donald Trump will assume office as the
President of the United States. He has mentioned that he wants Medicare (a
national social insurance program) to directly negotiate the price it pays for prescription drugs.
Medicare provides health insurance to Americans aged 65 or more, who
have worked and paid into the system through the payroll tax. It also provides
health insurance to younger people with some disabilities or end-stage renal
disease and amyotrophic lateral sclerosis.
In 2015, Medicare provided health insurance to over 55 million Americans — including 46 million people aged 65 or more, and nine million younger people.
As we flag off the New Year, PharmaCompass
provides insights into drug prices and prescription patterns in the US in order
to help professionals make informed decisions. We believe that the cost of
medicines in the US, which have been a subject of much public outcry and
discussions in the recent years, will continue to be scrutinized during 2017.
Medicare data for 2014
Medicare Part D, also known as the Medicare prescription drug benefit — the program which subsidizes the costs of prescription drugs and prescription drug insurance premiums for Medicare beneficiaries — published a data set (for calendar year 2014) which contains information from over one million healthcare providers
who collectively prescribed approximately US $121 billion worth of prescription
drugs paid for under this program.
For each prescriber and drug, the dataset
includes the total number of prescriptions that were dispensed (including
original prescriptions and any refills), and the total drug cost.
The total drug cost includes the ingredient cost of the medication, dispensing fees, sales tax, and any applicable administration fees. It’s based on the amounts paid by the Part D plan, the Medicare beneficiary, other government subsidies, and any other third-party payers (such as employers and liability insurers).
The total drug cost does not reflect any manufacturer rebates paid to Part D plan sponsors through direct and indirect remuneration or point-of sale rebates. In order to protect the beneficiary’s privacy, the Centers for Medicare & Medicaid Services (CMS) did not
include information in cases where 10 or fewer prescriptions were dispensed.
Top
Ten Drugs by Cost, 2014 [Most expensive for Medicare]
Drug Name
Total Claim Count
Beneficiary Count
Prescriber Count
Total Drug Cost
Sofosbuvir
109,543
33,028
7,323
$3,106,589,192
Esomeprazole Magnesium
7,537,736
1,405,570
286,927
$2,660,052,054
Rosuvastatin Calcium
9,072,799
1,752,423
266,499
$2,543,475,142
Aripiprazole
2,963,457
405,048
130,933
$2,526,731,476
Fluticasone/Salmeterol
6,093,354
1,420,515
281,775
$2,276,060,161
Tiotropium Bromide
5,852,258
1,211,919
253,277
$2,158,219,163
Lantus
Solostar
(Insulin Glargine)
4,441,782
972,882
224,710
$2,016,728,436
Sitagliptin Phosphate
4,495,964
789,828
190,741
$1,775,094,282
Lantus
(Insulin Glargine)
4,284,173
787,077
223,502
$1,725,391,907
Lenalidomide
178,373
27,142
9,337
$1,671,610,362
View the Medicare Part D National Prescriber Summary Report, Calendar Year 2014 (Excel version available) for FREE!
Top
Ten Drugs by Average Cost per Claim, 2014 [Most expensive drugs]
Drug Name
Total Claim Count
Beneficiary Count
Prescriber Count
Total Drug Cost
Average Cost Per Claim
Adagen
13
$1,224,835
$94,218
Elaprase
100
$6,560,225
$65,602
Cinryze
1,820
194
196
$96,155,785
$52,833
Carbaglu
60
$2,901,115
$48,352
Naglazyme
129
$6,189,045
$47,977
Berinert
538
73
68
$25,685,311
$47,742
Firazyr
1,568
269
232
$70,948,143
$45,248
H.P. Acthar
9,611
2,932
1,621
$391,189,653
$40,702
Procysbi
314
41
47
$12,542,911
$39,946
Folotyn
15
$598,210
$39,881
Top
Ten Drugs by Claims, 2014 [Most Commonly Used by Patients]
Generic Name
Total Claim Count
Beneficiary Count
Prescriber Count
Total Drug Cost
Lisinopril
38,278,860
7,454,940
464,747
$281,614,340
Levothyroxine Sodium
37,711,869
6,245,507
416,518
$631,855,415
Amlodipine Besylate
36,344,166
6,750,062
451,350
$303,779,661
Simvastatin
34,092,548
6,768,159
387,651
$346,677,118
Hydrocodone-Acetaminophen
33,446,696
8,005,790
677,865
$676,296,988
Omeprazole
33,032,770
6,707,964
475,122
$529,050,385
Atorvastatin Calcium
32,603,055
6,740,061
419,327
$747,635,818
Furosemide
27,133,430
5,176,582
456,047
$135,710,772
Metformin HCl
23,475,787
4,509,978
364,273
$203,948,989
Gabapentin
22,143,641
4,298,609
486,754
$492,557,255
View the Medicare Part D National Prescriber Summary Report, Calendar Year 2014 (Excel version available) for FREE!
Top
Ten Drugs by Prescribers, 2014 [Most Popular with Doctors]
Generic Name
Total Claim Count
Beneficiary Count
Prescriber Count
Total Drug Cost
Hydrocodone/Acetaminophen
33,446,696
8,005,790
677,865
$676,296,988
Ciprofloxacin HCl
7,253,018
4,926,835
568,201
$46,728,353
Amoxicillin
6,298,980
4,384,899
557,614
$31,193,739
Cephalexin
5,040,219
3,529,303
557,048
$36,987,401
Azithromycin
7,339,954
5,274,010
544,625
$70,699,119
Prednisone
11,032,986
4,505,821
536,108
$86,537,932
Tramadol HCl
14,250,227
4,272,724
515,816
$125,343,514
Sulfamethoxazole /Trimethoprim
4,833,758
3,090,944
500,790
$29,231,511
Gabapentin
22,143,641
4,298,609
486,754
$492,557,255
Amoxicillin/Potassium Clav
3,551,452
2,710,244
478,361
$61,713,432
The findings from CMS
data
The CY 2014 data represented a 17 percent
increase compared to the 2013 data set and a substantial part of the total estimated prescription drug spending (as estimated by the Department of Health and Human Services Office of the Assistant Secretary for Planning and Evaluation, or ASPE) in the United States — at about US $ 457 billion in 2015, which was 16.7 percent of the overall personal healthcare services.
Of that US $ 457 billion, US $ 328 billion (71.9 percent) was for retail
drugs and US $ 128 billion (28.1 percent) was for non-retail drugs.
The drug pricing process in the US is complex and
reflects the influence of numerous factors, including manufacturer list prices,
confidential negotiated discounts and rebates, insurance plan benefit designs,
and patient choices.
An IMS study found that across 12 therapy classes widely used in Medicare Part D,
medicine costs to plans and patients in Medicare Part D are 35 percent below
list prices.
View the Medicare Part D National Prescriber Summary Report, Calendar Year 2014 (Excel version available) for FREE!
While the CMS does not
currently have an established formulary, Part D drug coverage excludes drugs
not approved by the US Food and Drug Administration, those prescribed for off-label
use, drugs not available by prescription for
purchase in the US, and drugs for which payments would be available under Parts
A or B of Medicare.
Part D coverage
excludes drugs or classes of drugs excluded from Medicaid coverage,
such as:
Drugs used for anorexia, weight loss, or weight gain
Drugs used to promote fertility
Drugs used for erectile dysfunction
Drugs used for cosmetic purposes (hair growth, etc.)
Drugs used for the symptomatic relief of cough and colds
Prescription vitamins and mineral products, except prenatal vitamins and fluoride preparations
Drugs where the manufacturer requires (as a condition of sale) any associated tests or monitoring services to be purchased exclusively from that manufacturer or its designee
Our view
The Medicare program is designed such that the
federal government is not permitted to negotiate prices of drugs with the drug
companies, as federal agencies do under other programs.
For instance, the Department of Veterans Affairs — which is allowed to negotiate drug prices and establish a formulary — has been estimated to pay (on an average) between 40 to 58 percent less for drugs, as opposed to Medicare Part D.
If Trump administration kick starts direct
negotiations on Medicare drug prices with drug companies, 2017 will surely turn
out to be a year for the pharmaceutical industry to remember.
View the Medicare Part D National Prescriber Summary Report, Calendar Year 2014 (Excel version available) for FREE!
Impressions: 7923
https://www.pharmacompass.com/radio-compass-blog/drug-costs-and-prescription-trends-in-the-united-states-analyzing-medicare-s-121-billion-spend
#PharmaFlow by PHARMACOMPASS
05 Jan 2017

With Novartis shutting two plants in Germany and one in India by 2016-end, the global reliance on China for bulk drugs has increased even further, raising serious concerns over safety, supplies and national security. Which
plants? Last week, Novartis announced it will be shutting three plants of its generic business – Sandoz – by the end of 2016. The first plant is in India and the other two are located in Germany, in Gerlingen and Frankfurt. Frankfurt,
manufacturer of a key antibiotic intermediateThe Frankfurt plant is where Sandoz manufactures
7-ACA
(7-aminocephalosporanic acid), the core chemical structure (building block)
for producing a whole host of cephalosporin antibiotics. The reason given for closure -- prices of the cephalosporin active pharmaceutical ingredients (APIs) and intermediates have collapsed as Asian competitors have dumped excess capacity on the market. The shutdown of the Frankfurt facility
means that the global reliance on China for APIs, used to produce antibiotics
(such as cephalosporin) and especially
7-ACA, will increase only further. Chinese
APIs are already a security threat for India India produces a third of the world's
medicines, mostly in the form of generic drugs. However, according to an Oct 2014 report
by a Boston Consulting Group (BCG) and Confederation of Indian Industry (CII), more
than 90 percent of the key raw materials (intermediates and APIs) that go into
making at least 15-odd essential drugs come from China.The drugs listed include the most commonly used painkiller such as paracetamol, aspirin; antibiotics such as amoxicillin and ampicillin, cephalexin, cefaclor, ciprofloxacin, ofloxacin, levofloxacin; first line diabetes drug metformin; and antacid ranitidine. There are no domestic producers left for many drugs such as penicillin-G, and its derivative 6-aminopenicillanic acid, or 6-APA.Since India is still receiving a large quantity of 7-ACA from Germany (confirmed by the import statistics available on the PharmaCompass database), 7-ACA and its derivatives were not mentioned in this report.As per news reports, the Indian government
is now worried about over-dependence on imports from China. "Any
deterioration in relationship with China can potentially result in severe
shortages in the supply of essential drugs to the country. Additionally, China
could easily increase prices of some of these drugs where it enjoys virtual
monopoly," said Bart Janssens, partner, BCG, in a news
report published in The Economic Times. Recognizing the national healthcare
security challenge facing India, the Department of Pharmaceuticals (DoP) has
decided to declare the year 2015 as ‘Year of Active Pharmaceutical Ingredients.’ As part of this initiative, the Indian government intends
to build
cluster parks to boost India’s self-reliance on Chinese imports. Quality,
environmental concerns over Chinese AntibioticsChinese supplies of 7-ACA have been plagued
with multiple issues in the past. In 2012, for instance, several Chinese drug
companies were accused of manufacturing 7-ACA using contaminated ‘gutter oil’, instead of more
expensive soybean oil. Gutter oil is reprocessed oil manufactured from waste oil and animal fat collected from restaurants’ fryers, drains, grease traps and slaughterhouses. Chinese restaurants can get through a lot of cooking oil and this waste oil fuels a highly profitable gutter oil black market as there are few other outlets, such as biofuel production, for this by-product.Similarly, antibiotic pollution in the rivers of China is a serious cause of concern for the Chinese. Our previous analysis, “Antibiotic
resistant superbugs: deadlier than cancer and closer to you than you think” provides a detailed overview regarding the challenge being faced. However, with growing focus on antibiotic pollution in China, a shutdown of factories failing pollution norms would be a severe setback for the global antibiotic supply chain. In addition to these challenges, quality concerns have been raised during international regulatory inspections of some of the leading antibiotic producers in China, like Zhuhai
United and North
China Pharmaceutical Company. South
African stock outs of essential drugs a global concernThe outcomes of these challenges are already being felt in countries such as South Africa which are facing an acute shortage of critical drugs. According to a report
published in Groundup, drug shortages in South Africa’s health facilities have become a crisis. The story mentioned the situation in a hospital (Stanger Hospital) in Ilembe District KwaZulu Natal, where 200 products were out of stock. These included various doses of morphine, some antibiotics and antiretrovirals, especially paediatric ones, used to treat HIV. “About a hundred patients per week are going without ranitidine which prevents stomach ulcers. Several Ilembe facilities are even out of stock of paracetamol tablets,” the Groundup report said. There are multiple reasons for the drug stock
outs. However, unprofitability because old, off-patent products are being sold by
manufacturers at prices very close to the cost of production has played a major
role. Firms are abandoning such products and seeking higher return
alternatives. In addition, due to quality failures suppliers are unable to provide lifesaving medications to the South African population. Our
ViewThe problems of stock outs and quality concerns in South Africa can easily expand across the world and can’t be addressed until the global pharmaceutical industry reduces its reliance on China for bulk drugs and intermediates. It remains to be seen if the threat to the global supply chain will make Novartis reconsider its decision or drive a national government to buy the Frankfurt facility.
Impressions: 7491
https://www.pharmacompass.com/radio-compass-blog/novartis-plant-shut-down-creates-urgency-to-find-alternatives-to-chinese-apis
#PharmaFlow by PHARMACOMPASS
30 Jul 2015

