







Acquisitions and spin-offs dominated headlines in 2019 and the tone was set very early with Bristol-Myers Squibb acquiring
New Jersey-based cancer drug company Celgene in a US$ 74 billion deal announced on
January 3, 2019. After factoring
in debt, the deal value ballooned to about US$ 95 billion, which according
to data compiled by Refinitiv, made it the largest healthcare deal on
record.
In the summer, AbbVie Inc,
which sells the world’s best-selling drug Humira, announced its acquisition of Allergan Plc, known for Botox and other cosmetic
treatments, for US$ 63 billion. While the companies are still awaiting
regulatory approval for their deal, with US$ 49 billion in combined 2019
revenues, the merged entity would rank amongst the biggest in the industry.
View Our Interactive Dashboard on Top drugs by sales in 2019 (Free Excel Available)
The big five by pharmaceutical sales — Pfizer,
Roche, J&J, Novartis and Merck
Pfizer
continued
to lead companies by pharmaceutical sales by reporting annual 2019 revenues of
US$ 51.8 billion, a decrease of US$ 1.9 billion, or 4 percent, compared to
2018. The decline was primarily attributed to the loss of exclusivity of Lyrica in 2019,
which witnessed its sales drop from US$ 5 billion in 2018 to US$ 3.3 billion in
2019.
In 2018, Pfizer’s then incoming CEO Albert Bourla had mentioned that the company did not see the need for any large-scale M&A activity as Pfizer had “the best pipeline” in its history, which needed the company to focus on deploying its capital to keep its pipeline flowing and execute on its drug launches.
Bourla stayed true to his word and barring the acquisition of Array Biopharma for US$ 11.4 billion and a spin-off to merge Upjohn, Pfizer’s off-patent branded and generic established medicines business with
Mylan, there weren’t any other big ticket deals which were announced.
The
Upjohn-Mylan merged entity will be called Viatris and is expected to have 2020
revenues between US$ 19 and US$ 20 billion
and could outpace Teva to
become the largest generic company in the world, in term of revenues.
Novartis, which had
followed Pfizer with the second largest revenues in the pharmaceutical industry
in 2018, reported its first full year earnings after spinning off its Alcon eye
care devices business division that
had US$ 7.15 billion in 2018 sales.
In 2019,
Novartis slipped two spots in the ranking after reporting total sales of US$
47.4 billion and its CEO Vas Narasimhan continued his deal-making spree by buying New
Jersey-headquartered The Medicines Company (MedCo) for US$ 9.7
billion to acquire a late-stage cholesterol-lowering
therapy named inclisiran.
As Takeda Pharmaceutical Co was
busy in 2019 on working to reduce its debt burden incurred due to its US$ 62
billion purchase of Shire Plc, which was announced in 2018, Novartis also purchased
the eye-disease medicine, Xiidra, from the Japanese drugmaker for US$ 5.3 billion.
Novartis’ management also spent a considerable part of 2019 dealing with data-integrity concerns which emerged from its 2018 buyout of AveXis, the
gene-therapy maker Novartis had acquired for US$ 8.7 billion.
The deal gave Novartis rights to Zolgensma,
a novel treatment intended for children less than two years of age with the
most severe form of spinal muscular atrophy (SMA). Priced at US$ 2.1 million,
Zolgensma is currently the world’s most expensive drug.
However,
in a shocking announcement, a month after approving the drug, the US Food and
Drug Administration (FDA) issued a press release on
data accuracy issues as the agency was informed by AveXis that
its personnel had manipulated data which
the FDA used to evaluate product comparability and nonclinical (animal)
pharmacology as part of the biologics license application (BLA), which was
submitted and reviewed by the FDA.
With US$
50.0 billion (CHF 48.5 billion) in annual pharmaceutical sales, Swiss drugmaker
Roche came in at number two position in 2019
as its sales grew 11 percent driven by
its multiple sclerosis medicine Ocrevus, haemophilia drug Hemlibra and cancer medicines Tecentriq and Perjeta.
Roche’s newly introduced medicines generated US$ 5.53 billion (CHF 5.4 billion) in growth, helping offset the impact of the competition from biosimilars for its three best-selling drugs MabThera/Rituxan, Herceptin and Avastin.
In late 2019, after months of increased
antitrust scrutiny, Roche completed
its US$ 5.1 billion acquisition of Spark Therapeutics to strengthen its presence in
gene therapy.
Last year, J&J reported almost flat worldwide sales of US$ 82.1 billion. J&J’s pharmaceutical division generated US$ 42.20 billion and its medical devices and consumer health divisions brought in US$ 25.96 billion and US$ 13.89 billion respectively.
Since J&J’s consumer health division sells analgesics, digestive health along with beauty and oral care products, the US$ 5.43 billion in consumer health sales from over-the-counter drugs and women’s health products was only used in our assessment of J&J’s total pharmaceutical revenues. With combined pharmaceutical sales of US$ 47.63 billion, J&J made it to number three on our list.
While the sales of products like Stelara, Darzalex, Imbruvica, Invega Sustenna drove J&J’s pharmaceutical business to grow by 4 percent over 2018, the firm had to contend with generic competition against key revenue contributors Remicade and Zytiga.
US-headquartered Merck, which is known as
MSD (short for Merck Sharp & Dohme) outside the United States and
Canada, is set to significantly move up the rankings next year fueled by its
cancer drug Keytruda, which witnessed a 55
percent increase in sales to US$ 11.1 billion.
Merck reported total revenues of US$ 41.75 billion and also
announced it will spin off its women’s health drugs,
biosimilar drugs and older products to create a new pharmaceutical
company with US$ 6.5 billion in annual revenues.
The firm had anticipated 2020 sales between US$ 48.8 billion and US$ 50.3 billion however this week it announced that the coronavirus pandemic will reduce 2020 sales by more than $2 billion.
View Our Interactive Dashboard on Top drugs by sales in 2019 (Free Excel Available)
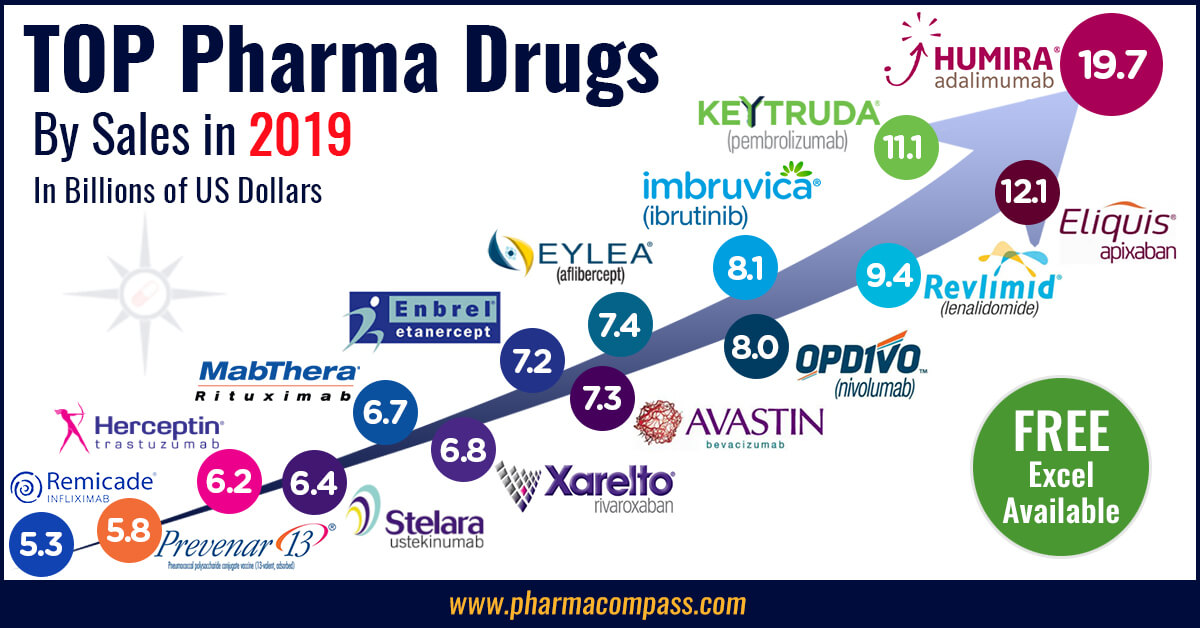
Humira holds on to remain world’s best-selling drug
AbbVie’s acquisition of Allergan comes as the firm faces the expiration of patent protection for Humira, which brought in a staggering US$ 19.2 billion in sales last year for
the company. AbbVie has failed to successfully acquire or develop a major new
product to replace the sales generated by its flagship drug.
In 2019, Humira’s US revenues increased 8.6 percent to US$ 14.86 billion while internationally, due
to biosimilar competition, the sales dropped 31.1 percent to US$ 4.30 billion.
Bristol Myers Squibb’s Eliquis, which is also marketed by Pfizer, maintained its number two position
and posted total sales of US$ 12.1 billion, a 23 percent increase over 2018.
While Bristol Myers Squibb’s immunotherapy treatment Opdivo, sold in partnership with Ono in Japan, saw sales increase from US$ 7.57 billion to US$ 8.0 billion, the growth paled in comparison to the US$ 3.9
billion revenue increase of Opdivo’s key immunotherapy competitor Merck’s Keytruda.
Keytruda took the number three spot in drug sales that
previously belonged to Celgene’s Revlimid, which witnessed a sales decline from US$ 9.69 billion to US$ 9.4 billion.
Cancer treatment Imbruvica, which is marketed
by J&J and AbbVie, witnessed a 30 percent increase in sales. With US$ 8.1
billion in 2019 revenues, it took the number five position.
View Our Interactive Dashboard on Top drugs by sales in 2019 (Free Excel Available)
Vaccines – Covid-19 turns competitors into partners
This year has been dominated by the single biggest health emergency in years — the novel coronavirus (Covid-19) pandemic. As drugs continue to fail to meet expectations, vaccine development has received a lot of attention.
GSK reported the highest vaccine sales of all drugmakers with
total sales of US$ 8.4 billion (GBP 7.16 billion), a significant portion of its
total sales of US$ 41.8 billion (GBP 33.754 billion).
US-based Merck’s vaccine division also reported a significant increase in sales to US$ 8.0 billion and in 2019 received FDA and EU approval to market its Ebola vaccine Ervebo.
This is the first FDA-authorized vaccine against the deadly virus which causes
hemorrhagic fever and spreads from person to person through direct contact with
body fluids.
Pfizer and Sanofi also reported an increase in their vaccine sales to US$ 6.4
billion and US$ 6.2 billion respectively and the Covid-19 pandemic has recently
pushed drugmakers to move faster than ever before and has also converted
competitors into partners.
In a rare move, drug behemoths — Sanofi and GlaxoSmithKline (GSK) —joined hands to develop a vaccine for the novel coronavirus.
The two companies plan to start human trials
in the second half of this year, and if things go right, they will file
for potential approvals by the second half of 2021.
View Our Interactive Dashboard on Top drugs by sales in 2019 (Free Excel Available)
Our view
Covid-19 has brought the world economy to a grinding halt and shifted the global attention to the pharmaceutical industry’s capability to deliver solutions to address this pandemic.
Our compilation shows that vaccines and drugs
for infectious diseases currently form a tiny fraction of the total sales of
pharmaceutical companies and few drugs against infectious diseases rank high on
the sales list.
This could well explain the limited range of
options currently available to fight Covid-19. With the pandemic currently infecting
over 3 million people spread across more than 200 countries, we can safely
conclude that the scenario in 2020 will change substantially. And so should our
compilation of top drugs for the year.
View Our Interactive Dashboard on Top drugs by sales in 2019 (Free Excel Available)
Impressions: 54752
https://www.pharmacompass.com/radio-compass-blog/top-drugs-and-pharmaceutical-companies-of-2019-by-revenues
#PharmaFlow by PHARMACOMPASS
29 Apr 2020

Divi's Laboratories — an Indian active pharmaceutical ingredient (API) manufacturer and until recently the darling of the Indian bourses — received another setback this week.
The US Food and Drug Administration (FDA) placed its Unit
II, located in Visakhapatnam, on its import alert list for “refusing FDA foreign establishment inspection”
as also for “not meeting drug GMPs” (good manufacturing practices).
According to the FDA website “the refusal to permit inspection of a foreign facility or provide reasonable access to FDA’s inspectional personnel, combined with other evidence, provides an appearance that the firm’s products are manufactured, processed, or packed under insanitary conditions.” The firm is considered to have refused the FDA inspection.
This news comes as a surprise, as it adds an additional dimension to the problems that the FDA encountered at Divi’s facilities.
PharmaCompass
had
previously shared news that Health Canada had placed the company on its inspection tracker after data integrity and general GMP observations were reported by its “regulatory partner(s)”.
According to
media reports, the firm was inspected by the US FDA from November 29 to
December 6, 2016, and the regulators had issued an 18-page long Form 483 with five observations.
Second Divi’s group firm to refuse inspection
The news comes a few months after its affiliate – Divi’s Pharmaceutical Private Ltd was placed on FDA’s Import Alert List for refusing an inspection by the US
FDA.
The two
facilities of Divi’s Pharmaceutical that were placed on the FDA’s Red List were Divi Towers in Hyderabad, and a facility in Medak district, Telangana. Divi Towers is also the corporate headquarters of Divi’s Laboratories.
Divi’s Laboratories’ Unit-II is a major producer of APIs and a key supplier to leading companies around the world. The FDA has excluded some intermediates and the following APIs from the import alerts – Levetiracetam, Gabapentin, Lamotrigine, Capecitabine, Naproxen sodium , Raltegravir potassium and Atovaquone.
The exemptions did not help as far as the stock market was concerned. Divi’s stock price, which has already been under significant pressure after news of the inspection initially broke out in December, tanked another 20 percent on Tuesday.
Our view
While the details are yet to emerge on the exact nature of problems which the US FDA inspectors uncovered and encountered at Divi’s Laboratories Unit II, it is clear that Divi’s has a long road ahead insofar as regulatory compliance is concerned.
Impressions: 3525
https://www.pharmacompass.com/radio-compass-blog/divi-s-labs-on-fda-s-import-alert-list-but-did-it-refuse-an-inspection
#PharmaFlow by PHARMACOMPASS
23 Mar 2017

Teva Pharmaceutical Industries, Ltd., which acquired Cephalon in 2012, will make a total payment of $1.2 billion as part of a ‘pay-for-delay’ settlement reached with the Federal Trade Commission (FTC) last week.
What exactly did Cephalon, for which Teva paid $6.8 billion, do so wrong? Isn’t ‘pay-for-delay’ common practice in the pharmaceutical industry?
First of all what is a
pay-for-delay?
‘Pay for delay’ or reverse payment patent settlements, are agreements where the brand name drug manufacturer compensates generics, not to market the generic product for a specific period of time.
These settlements allow the brand manufacturers to extend their
patent monopolies and according to an FTC study, these deals
cost consumers and taxpayers $3.5 billion in higher drug costs every year.
What exactly happens and
why is it a big deal now?
Cephalon allegedly paid four generic drug companies (Teva, Ranbaxy Pharmaceuticals, Mylan Pharmaceuticals, and Barr Laboratories), over $300 million in total. In return the generics agreed to drop their patent challenges and forgo marketing of their generic versions of Cephalon’s blockbuster sleep-disorder drug Provigil, for six years, until April 2012.
An extended monopoly for Provigil, in the absence of generic competition, was “$4 billion in sales that no one expected”, the CEO of Cephalon reportedly said when the deal was struck.
While in Europe, regulators have been going after pay-for-delay cases for years, it was only as recently as 2013, in FTC v. Actavis, that the U.S. Supreme Court made clear that reverse payment patent settlements are subject to the same antitrust rules that govern general U.S. business conduct.
The payment made by Teva will compensate purchasers, including drug wholesalers, pharmacies, and insurers, who overpaid because of Cephalon’s illegal conduct, is the first positive outcome for the FTC after the Supreme Court ruling.
How common are ‘pay-for-delay’ settlements?
Based on data provided by the FTC, for the past few years, more
than 100 settlements are reached annually between brand and generic
pharmaceutical companies.
Over 30% of these settlements have the potential of being ‘pay-for-delay’ agreements.
Table// Potential
pay-for-delay settlements reached between brand and generic companies:
Financial Year
2004
2005
2006
2007
2008
2009
2010
2011
2012
2013
Final Settlements:
between brand and generic companies
14
11
28
33
66
68
113
156
140
145
Involving First Generic Filing
8
5
11
16
29
32
49
54
43
41
Potential Pay-for-Delay:
Involving First Generic Filing
2
9
11
13
15
26
18
23
13
Settlements
3
14
14
16
19
31
28
40
29
How severe are the penalties for ‘pay-for-delay’ settlements in Europe?
The European Commission has
fined Johnson
& Johnson (J&J) just under 10.8 million
euros and Novartis 5.49 million euros, after discovering a ‘pay-for-delay’ deal on the painkiller Duragesic (fentanyl).
The amount pales in comparison to
the whopping €428m fine on Servier and several other companies (Niche/ Unichem; Matrix, which is now part of Mylan; Teva; Krka and Lupin) for conspiring to delay generics of the widely-used blood pressure drug Coversyl/ Aceon (perindopril).
In yet another settlement, agreements which operated in 2002 and
2003 between the Danish originator Lundbeck, and other
generic companies, resulted in Euro
146 million in fines.
What should we expect in the future?
Based on an FTC
presentation made in September 2014, they highlighted 19 Cases to Watch, which has them targeting almost every
major brand and generic pharmaceutical company. However, with the complexities
involved, this list is continuously evolving:
The
cases (by name of the brand product) Actos,
Adderall,
Aggrenox,
AndroGel,
Cipro,
Effexor,
K-Dur, Lamictal, Lidoderm,
Lipitor,
Loestrin,
Nexium,
Niaspan,
Opana,
Provigil,
Skelaxin,
Solodyn,
Wellbutrin.The
brand companies involvedAbbvie,
Abbott,
AstraZeneca,
Bayer,
Besins,
Biovail,
Boehringer,
Cephalon,
Endo,
GlaxoSmithKline,
King,
Medicis,
Pfizer,
Shire,
Schering,
Takeda,
Warner
Chilcott, Wyeth.The
generic companies Actavis
, Barr,
Duramed,
Dr. Reddy’s, HMR, Impax,
Lupin,
Mutual,
Mylan, Par, Perrigo,
Ranbaxy,
Rugby, Sandoz,
Teva,
Upsher
Smith.
Our view:
Pharmaceutical companies,
lawyers and the FTC will be busy for the coming few years, since there are a
series of suits, which will be challenging settlements reached between brand
and generic pharmaceutical companies.
While patents
provide temporary monopolies to promote innovation, brand drug manufacturers
will need to resort to more innovative ways of sustaining their profits.
Click here and learn about the different strategies adopted in the United States to block generics?
Impressions: 3400
https://www.pharmacompass.com/radio-compass-blog/haunted-teva-s-1-2-billion-pay-for-delay-penalty-which-companies-will-get-hit-next
#PharmaFlow by PHARMACOMPASS
04 Jun 2015

When a generic drug comes to the U.S.
market, sales of brand drugs crash. The drop is more than 80% by the time a second- or third- generation
generic arrives.For brand companies, used to high profits for years, the imminent generic threat leads to an aggressive search for ‘solutions’, and creative strategies to maximize returns from their products. What kind of blocking tactics are
used to stop generic competition?In an attempt to delay generic competition, here are some of the
commonly used approaches. 1/ Go legal:While a new drug patent
is difficult to invent around, there are brand drugs with weak
patents which may not withstand scrutiny. In such cases, the
brand drug manufacturer files a patent infringement complaint with the FDA. The
mere filing of the complaint triggers an automatic 30-month stay of FDA
approval, as per the provisions of the Hatch-Waxman Act. Understanding the Hatch-Waxman Act:In
1984, a United States federal law was designed
to encourage the manufacture of generic
drugs by pharmaceutical industry. The amendments of the Act protect the first generic (the ‘first-filer’) to challenge the brand’s patent, by mandating that the FDA not approve any additional generic competitors until 180 days, after the first-filer launches its product. 2/ Sample obstruction:Brands attempt to prevent
generic firms from accessing samples of the brand drug necessary to perform equivalence studies. The reason provided is
that the brand drug falls under restricted distribution, part of the FDA-mandated
programs, known as Risk Evaluation and Mitigation Strategies (REMS). Brand firms also
implement distribution restrictions for drugs that are not subject to REMS.3/ Destroy the product:Brand name pharmaceutical companies try to preserve the profits on a patented drug by making modest reformulations that offer little or no therapeutic advantages. This tactic is known as ‘product-switching’ or ‘product hopping’. In addition, prior to a generic launch, the brand drug simply withdraws its original product forcing patients to switch to the reformulated drug, so consumers don’t benefit from generic competition of the old version of the drug. Actavis’ ongoing Namenda litigation covers this example
perfectly.4/ Change the rule of the game:In order to overcome the
patents of the brand drugs, generic medicines are manufactured slightly
differently, when compared with the brand product. Citizen petitions are
filed with the FDA, at the behest of brand manufacturers, questioning the
safety of the generic drug, due to the difference between the brand and generic
products. A successful petition,
changes the regulatory requirements, and makes it harder for generics to obtain
FDA approval. The brand manufacturers were filing so many frivolous
citizen petitions that the FDA has been denying
them in record numbers. In the event, generic companies do manage to make significant inroads, and threaten the brand drug’s monopoly, there is a ‘pay-for-delay’ playbook. How does the ‘pay-for-delay’ game get played?Settlements are reached between brand and generic manufacturers in which
the brand incentivizes the generic not to market their products. The incentives can involve any of the following options:- Cash payment made from the brand to the generic that claims to reimburse some or all of the generic’s litigation fees.- A side business deal
between brand and generic manufacturers such as an agreement to buy active
pharmaceutical ingredient (API) from the generic manufacturer, even though the
brand has adequate supply of the API for their own needs (e.g. AstraZeneca, Ranbaxy’s Nexium deal).- Brand manufacturer promises not
to market an Authorized Generic (AG) in competition with the generic manufacturer’s product for some period of time. AGs are pharmaceutical products, which are approved as brand-name drugs,
but marketed as generic drugs. No authorized generics significantly reduce the
competition for the generic player allowing them to secure greater market share
and extract higher prices: e.g.
GlaxoSmithKline (GSK) paid Teva Pharmaceuticals to delay entry by promising
not to compete with authorized generic versions of the drug Lamictal.- Brand allows the generic to market an authorized generic of a different product: e.g. AbbVie’s Androgel case against Teva had Teva asking for supply of an authorized
generic of TriCor, a cholesterol drug with 2011 sales of more than $1 billion. - Other forms of compensation are offered to the generic patent
challenger. For example, an agreement containing a declining royalty structure in which, the intellectual property is
licensed by the brand to the generic. Alternativelly, a co-development deal can be struck for a new drug. Our view:The battle between brands and generics will continue for time to come,
and regardless of antitrust scrutiny, there will be a high degree of innovation
in the strategies devised by brand firms to maximize profits. However, drug companies aren’t the only ones innovating. Hayman Capital wins our vote for the most innovative approach taken. The hedge fund’s “Dispute the patent, short the stock” formula is designed to try and make money regardless of the outcome. How exactly the healthcare system benefits from these different approaches
is a completely different story!Click here and learn about the latest ‘pay-for-delay’ cases in Europe and America
Impressions: 2717
https://www.pharmacompass.com/radio-compass-blog/pharma-chess-strategies-adopted-in-the-united-states-to-block-generics
#PharmaFlow by PHARMACOMPASS
04 Jun 2015
Unrelated to the inspection of
the USFDA at the Dr. Reddys Srikakulam facility, Dr. Reddys sought permission from the Ministry of Environment,
Forests & Climate Change to expand
their drug and intermediate manufacturing at three locations.
All three chemical technical operation (CTO) units, CTO-I, CTO-II & CTO-III are located in Medak district and the announced planned capacity increases along with the anticipated capital investment were
Existing Capacity
Planned Capacity
Anticipated Investment
CTO I
14.7 TPM
45.5 TPM
Rs 30 crores
CTO II
21.9 TPM
68.9 TPM
Rs 45 crores
CTO - III
4.45 TPM
28.1 TPM
Rs 12 crores
*$1 million is approximately about Rs 6.2
crores & TPM is tons per month
In addition, the declaration given by Dr. Reddys also mentions the various products which will be produced at each facility (table below).
Needless to say, the plans are ambitious however with the growth witnessed by the Indian pharmaceutical industry over the past decade, one can understand Dr. Reddys commitment to investing further in their business.
Table Dr. Reddys production plans at various facilities
Product
Name
Planned
Capacity (TPM)
Facility
Location
Alendronate
Sodium Trihydrate
6.67
CTO
- III
Alfuzosin
2.33
CTO
- I
Altretamine
0.03
CTO
- I
Amlodipine
Besylate
33.33
CTO
- II
Amlodipine
Besylate
133.33
CTO
- III
Amlodipine
Besylate ( Ethyl 4 [2- (pthalamide)ethoxy] aceto acetate (TDM-2)
100
CTO
- II
Amlodipine
Maleate
30
CTO
- III
Amsacrine
0.07
CTO
- I
Anastrazole
0.83
CTO
- II
Aprepitant
3.33
CTO
- III
Aripiprazole
0.33
CTO
- II
Atomoxetine
1.67
CTO
- III
Atorvastatin
375.83
CTO
- II
Azacitidine
0.67
CTO
- I
Bicalutamide
0.03
CTO
- II
Bivalirudin
0.03
CTO
- II
Bivalirudin
Trifluoro Acetate
0.03
CTO
- I
Bortezomib
0.03
CTO
- I
Cabazitaxel
0.02
CTO
- I
Candesartan
cilexetil
6.67
CTO
- II
Cetirizine
Hydrochloride
66.67
CTO
- I
Cetirizine
16.67
CTO
- II
Ciprofloxacin
176.67
CTO
- II
Ciprofloxacin
HCl
533.33
CTO
- II
Ciprofloxacin Lactate
33.33
CTO
- II
Clopidogrel
Bisulfate
500
CTO
- I
Clopidogrel Premix
166.67
CTO
- II
Diluted
Everolimus 5% (Everolimus)
0.33
CTO
- II
Disodium
Pamidronate
0.33
CTO
- III
Docetaxel
1.9
CTO
- I
Dutasteride
3.33
CTO
- II
Esomeprazole
magnesium
66.67
CTO
- III
Ezetimibe
3.33
CTO
- II
Fexofenadine
Hydrochloride
500
CTO
- I
Finasteride
10
CTO
- II
Fluoxetine
110
CTO
- I
Fondaparinux
Sodium
0.33
CTO
- II
Galantamine
0.03
CTO
- II
Gemcitabine
13.33
CTO
- I
Glimepiride
13.33
CTO
- II
Imatinib
0.17
CTO
- I
Irinotecan
0.33
CTO
- I
Ketorolac
66.67
CTO
- II
Lacidipine
5
CTO
- III
Lamotrigine
33.33
CTO
- I
Lansoprozole
8.33
CTO
- III
Letrozole
0.03
CTO
- II
Levocetrizine
Di HCl
10
CTO
- III
Levofloxacin
200
CTO
- II
Lomustine
1.33
CTO
- I
Losartan
Postassium
150
CTO
- I
Meloxicam
0.03
CTO
- I
Memantine
HCl
3.33
CTO
- II
Mesalamine
0.03
CTO
- II
Metoprolol
Succinate
266.67
CTO
- II
Moxifloxacin
116.67
CTO
- II
Norfloxacin
0.03
CTO
- I
Omeprazole
133.33
CTO
- III
Omeprazole
Magnesium
50
CTO
- III
Omeprazole
Sodium
10
CTO
- III
Omerprazole Form B
33.33
CTO
- III
Paclitaxel
0.33
CTO
- I
Pantoprazole
Sodium
100
CTO
- III
paroxetine
HCl
0.03
CTO
- II
Pemetrexed
0.67
CTO
- I
Rabeprazole
Sodium
83.33
CTO
- III
Raloxifene
33.33
CTO
- II
Ramipril
100
CTO
- III
Repaglinide
6.67
CTO
- II
Rivastigmine
6.67
CTO
- II
Risperidone
13.33
CTO
- I
Rivastigmine
6.667
CTO
- I
Rizatriptan
Benzoate
1.33
CTO
- II
Rocuronium
Bromide
0.03
CTO
- II
Ropinrole
HCl
1.83
CTO
- III
Rosiglitazone
3.33
CTO
- II
Sparfloxacin
3.33
CTO
- I
Tacrolimus
5
CTO
- II
Tadalafil
3.33
CTO
- II
Telmisartan
100
CTO
- II
Temozolamide
0.03
CTO
- I
Terbinafine
HCl
133.33
CTO
- III
Tizanidine
HCl
16.67
CTO
- III
Topotecan
0.07
CTO
- I
valganciclovir
0.03
CTO
- I
Vardenafil
3.33
CTO
- II
Voriconazole
8.33
CTO
- III
Ziprasidone
Hydrochloride
100
CTO
- I
Zoledronic
acid
0.33
CTO
- III
Zolmitriptan
0.83
CTO
- I
Zonisamide
0.03
CTO
- II
Impressions: 3086
https://www.pharmacompass.com/radio-compass-blog/dr-reddy-s-expansion-plans-for-api-production
#PharmaFlow by PHARMACOMPASS
03 Apr 2015

